Dr Kirti Bushan
 Tobacco is currently labelled as “world epidemic” because it is principle cause of preventable, disease, disability and premature deaths worldwide. In the past, it was considered auspicious and used for medicinal and religious purposes. It took 500 hundred years to realise that it is a “killer”. The WHO estimated 4 million tobacco related death worldwide and in 2020 it is expected to double. Tobacco is a major cause of stroke, fatal heart attacks, raised blood pressure, suppressed immune functions, dull sense of smell and taste, wrinkles over skin, reduced stamina, emphysema, addiction, depression, fatigue and above all may cause cancer.
Tobacco is currently labelled as “world epidemic” because it is principle cause of preventable, disease, disability and premature deaths worldwide. In the past, it was considered auspicious and used for medicinal and religious purposes. It took 500 hundred years to realise that it is a “killer”. The WHO estimated 4 million tobacco related death worldwide and in 2020 it is expected to double. Tobacco is a major cause of stroke, fatal heart attacks, raised blood pressure, suppressed immune functions, dull sense of smell and taste, wrinkles over skin, reduced stamina, emphysema, addiction, depression, fatigue and above all may cause cancer.
Tobacco and Cancer risk
The risk of cancer in tobacco users is 3-13 times as compared to normal population. Tobacco and tobacco products increase the risk of number of cancers..According to American Institute of Cancer Research (AICR) there is a convincing evidence for a causal association between tobacco smoke and cancers of lung, oropharynx, larynx, esophagus, stomach, pancreas, kidneys and urinary bladder. For the rest of cancers, the causal association are termed either as probable, possible or unlikely. The causal association is probable for colorectal, prostate, cervical and liver cancers and possible for adrenal, gall bladder, genital and sinonasal cancers.
A large number of studies have shown that stopping smoking can greatly reduce the risk of smoking related cancers.. Cesation of smoking leads to decreasing risk by 50% after 10-15 years of cessation. Studies have also shown that it is never too late to quit as people who quit smoking even in their late sixties can experience health benefits and get valuable years of life.
Tobacco Car Cinogensis
The forms or types of tobacco used are: smoked form, e.g, cigarette, pipes, cigar ; smokeless form, e.g, gutka, zarda, snuff ; dark (black) form – air cured used in cigars, pipes ; and white (blonde) form – flue cured used in cigarettes.
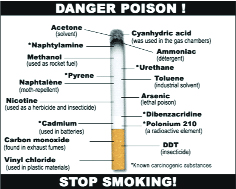
There are 4000 chemicals in tobacco with 100 identified poisons and 63 known carcinogens. Tobacco smoke is a heterogeneous aerosol formed due to incomplete combustion of tobacco leaf. The constituents of tobacco smoke include gas phase (90%) and particulate phase (10%).The gas phase contains carbon monoxide, hydrocyanic acid, acetaldehyde, acrolein, ammonia, formaldehyde, nitrosamine, hydrazine and vinyl chloride. The particulate phase contains TAR, polycyclic aromatic hydrocarbons (PAH), nicotine, phenol, cresol, ?-nephthylamine, benzopyreme, indole, carbazole and cartechol. These constituents have been proved to have carcinogenic effect.
Paan and Cancer Risk
Mostly in our country paan, a form of tobacco is used which is most common etiological factor in oral cavity cancers. The ingredients of paan are:- chuna (Limepaste) – lime contains calcium oxide or hydroxide ; supari – which is bettlenut ( arecanut) ; katha – it is a red solution ; and catechu which acts as astringent and disinfectant material. Chuna combines with supari (bettlenut) to form narcotic arecoline which is carcinogenic. Katha and catechu causes mucosal ulcerations, increase salivation and impart red colour to solution and creates an ideal environment for arecoline to execute its carcinogenic potential.
Second Hand Smoke
It refers to the involuntary nature of exposure in non smokers. Main carcinogen here is cotinine. Studies have shown that those expose to highest level of second hand smoke at work have twice the risk of lung cancer compare to those who are not. Second hand smoke contains over 50 known chemical carcinogens and cause lung cancer and coronary heart disease in non smokers. An estimated 3000 non smoking Americans dies of lung cancer per year.
Tobacco control strategies
Role of Clinician
. The clinicians roles in a community is very vital as majority of smokers visit physicians every year. Role of clinician is to follow 5A’s:-ask, assess, advice, assist and arrange.The physician needs to ASK smoker about history of smoking, likely level of nicotine addiction, level of smoking, interest in quitting and any quitting experience. A clinician must ASSESS will and desire of person to quit smoking. Third thing a clinician can do is ADVICE i.e, educate regarding benefits of cessation of smoking; explain physical, psychological, economical benefits of quitting; explain people about improvement in sensation of taste, smell, decrease risk of cardio pulmonary disease and decrease risk of cancers. A clinician must ASSIST in selection of a cessation plan – by self help, physician assisted, counselling session, psychological support or pharmaceutical therapy. A clinician must ARRANGE follow up contacts o monitor progress, deal with relapse and consider alternate methodology for cessation.
Pharmacotherapy
There are number of medications which can help the smoker quit. However they are not nearly more effective when used alone than they are in combination with counselling and support group. These medications include:-Mint snuff (A smokeless tobacco substitute), nicotine patches, nicotine gum (used to control sudden cravings) ; chantix – blocks nicotine receptors in brain and patients loose their craving for nicotine and even may develop repulsion to it ; nicotine replacement therapies (NRT) ; buproprion (anti depressants) ,; zyban – drug whose main effect is to control withdrawal symptoms works by affecting level of neutrotransmitters dopamine and nor-ephirine.
(The author is Consultant Surgical Oncologist at Asian Institute of Oncology, Lilawati hospital , Bombay hospital and S L Raheja (Fortis) hospital Mumbai )
Trending Now
E-Paper